
For decades we have heard that a child shouldn’t see an orthodontist until they lose all the baby teeth or reach 12 years old. However, modern dental science shifts this long-held mindset on age restriction. Early orthodontic treatment known as Phase 1 is not just about straight teeth. It is an effective approach that focuses on the skeletal structure of the jaw and development path of teeth. When the child’s jaw is in the growing stage, an orthodontist can easily achieve results that are quite impossible when the jaw is mature, such as correcting bite issues and guiding the proper alignment of teeth as they emerge.
The “Age 7” Rule: Why Timing is Everything
At age 7, the first permanent molars erupt, meaning the teeth create the “back bite,” which helps orthodontists to examine the front-to-back and side-to-side structure and relationship of the jaw. This is the blueprint for adult smiles. If the molars aren’t correct in childhood, it can affect the alignment of all teeth.
Another reason is many children have all the permanent front teeth by the age of 7, so the orthodontist finds it easy to detect crowding, overbites, or “trapped” teeth. Because the adult teeth are broad as compared to baby teeth they replace, this is the first real test of whether the child’s jaw is wide enough to accommodate their future smile.
At the age of 7, the jaw is still developing; the midline palatal suture of the mouth has not yet fused. This works as a golden opportunity where orthodontists can gently widen a narrow jaw by simply using a palatal expander. This process is much easier in childhood as compared to adulthood because, in adults, it requires surgery. At the age of 6 it is easy to move bones, but at the age of 17 orthodontists have to fight for them.

7 Red Flags: How to Tell if Your Child Needs an Evaluation
While only an orthodontist can confirm when the child needs evaluation, as a parent you can look for these seven clinical indicators:
Early or Late Loss of Baby Teeth: When your child has baby teeth, they work as space maintainers. If a child lost baby teeth to decay or trauma, the remaining teeth block the path for the permanent tooth. On the other hand, if baby teeth remain the same for a long time, then the adult teeth are forced to grow in the wrong direction.
Mouth breathing is a condition known as “long face syndrome.” It takes place when a person is unable to breathe easily from their nose, so they breathe from their mouth. Because the mouth remains open, the body is used to it and changes the way the face grows. It often causes crowded teeth.
Difficulty Chewing or Biting: If your child bites their cheek or struggles with hard food while eating, then it is a sign of a crossbite.
Crowding or “Blocked Out” Teeth: If there is no space between baby teeth, it means there is no room for adult teeth to grow. Adult teeth may come in at odd angles or become impacted within the jawbone.
Jaws that Shift or Make Sounds: When you notice there is a clicking sound when a child opens the mouth, it means there is a functional jaw discrepancy, which leads to TMJ dysfunction later in life.
Speech Impediments: There will also be some other sounds like lisps or whistling, which occur due to the tongue’s inability to sit correctly between teeth or palate because of an open narrow arch.
Thumb Sucking Past Age 5: Constant sucking habits can push the front teeth outside and narrow the upper jaw, which leads to dysfunction as the front doesn’t align with all the back teeth.

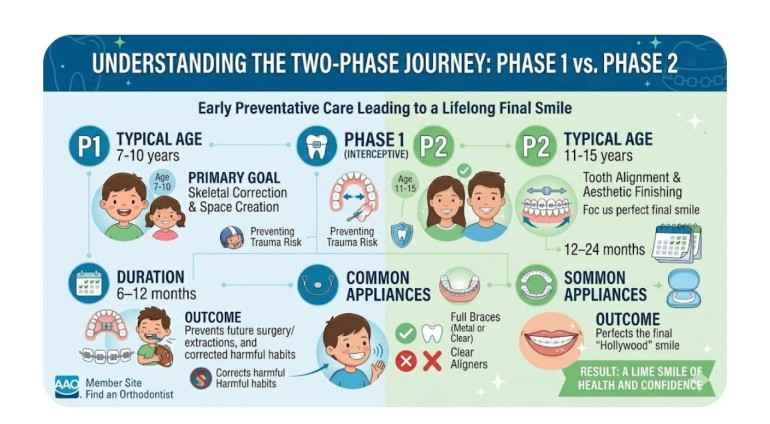
Phase 1 vs. Phase 2: Understanding the Two-Phase Journey
There are two different phases we need to understand for long-term planning because some parents think phase 1 is a long process and do twice the work, but in reality, each phase is working differently.
Beyond Straight Teeth: Improving Nasal Breathing and Sleep Quality
This is considered a most critical advancement in modern orthodontics. The roof of the mouth is also considered the floor of the nasal cavity. When your child has a high arched palate, it squeezes the nasal passages.
The Orthodontic-Airway Connection
The first thing used in phase 1 treatment is a palatal expander. The orthodontist uses this to widen the upper jaw, which leads to expanding the nasal floor and increasing the volume of the nasal airway.
The “Mouth Breathing” Cycle: When a child can’t breathe from their nose, they start doing it naturally from their mouth. This lowers the tongue position, which results in failure to support the upper jaw, resulting in more narrowing. However, people go for phase 1 because it breaks the cycle.
Children who breathe from their mouths find it difficult to sleep peacefully. They suffer from snoring and pediatric sleep apnea. When the airway gets opened, it can lead to better sleep, which is important for hormone production.
When a child is getting better sleep without any difficulty, it can lead to better focus and behavior. Many children today are misdiagnosed with ADHD; they are actually suffering from sleep-disordered breathing that can be easily treated by orthodontic expansion.
Is Early Treatment Always Necessary? (The “Wait and See” Approach)
Transparency plays an important role in these cases. To be honest, every child is different, which means not every child needs phase 1. Many children are better treated based on the “Growth and Guidance” approach. Orthodontists typically recommend against early intervention if:
- The issue is cosmetic and doesn’t involve the jaw bone.
- There is not a crowd, meaning enough space for adult teeth to grow and stay naturally.
- The bites (the teeth are naturally aligned) are healthy and functional.
What Happens in “Observation”?
If the orthodontist notices your child doesn’t need phase 1 treatment urgently, then they enter a wait-and-see phase. This isn’t just about waiting for the orthodontist to monitor the child’s teeth in
6–12 months to see the eruption of permanent teeth. Track baby teeth loss to make sure they fall in the correct order. Orthodontists also use low-dose 3D imaging if necessary to make sure the adult teeth aren’t stuck against the roots. They measure jaw growth to ensure it remains on track.
All these small observations can help in making decisions like whether your child needs braces or not! If yes, then at the exact right moment, not a moment too soon.
Common Appliances Used in Interceptive Orthodontics: A Technical Guide
Early treatment involves a full set of braces in very rare cases. The most common tools used in early treatment are as follows:
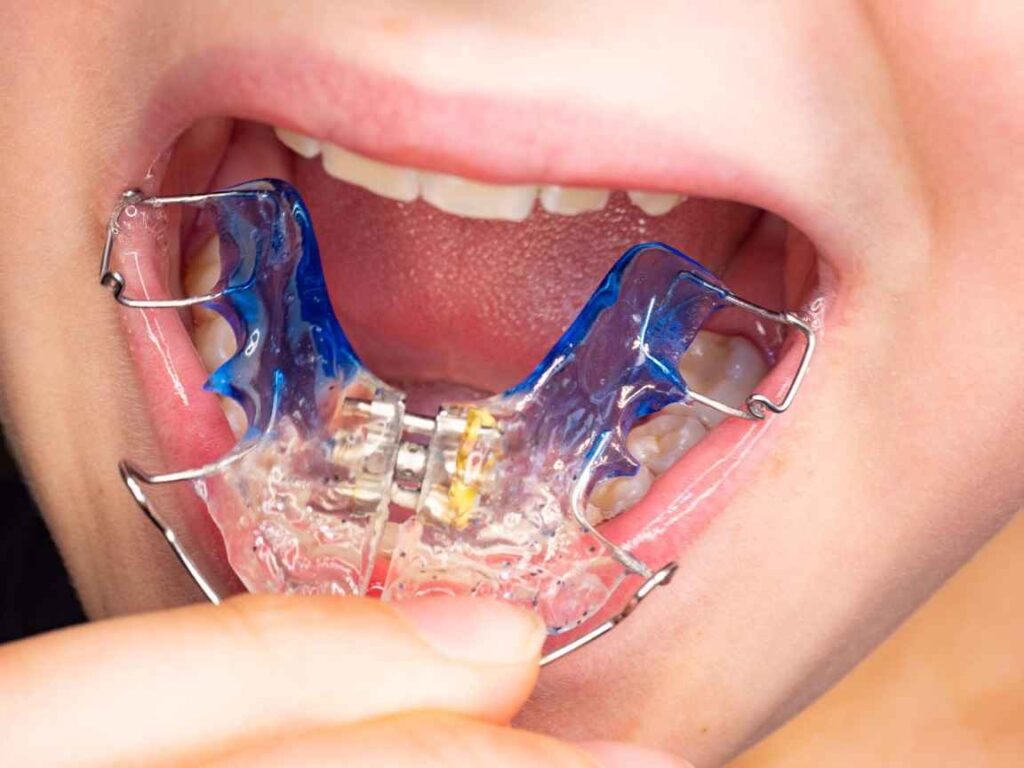
Palatal Expanders (The Most Common Tool)
It is a custom-made device that fits on upper molars. It has just one screw in the center that parents can easily turn at home with a customized key. Every time it turns, it creates a small amount of pressure on the two halves in the upper jaw, allowing them to grow wider apart. This is generally a safe and painless process because the growth plate hasn’t fused yet.
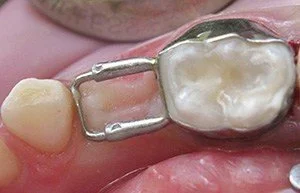
Space Maintainers (The Foundation Protectors)
If a baby tooth is lost early because of a cavity or any accident, then the space maintainers are used. There is a small metal ring and loop that helps in preventing the other teeth from taking the place of the lost one. If the space maintainer wasn’t used, the adult tooth underneath would have no place to go and might be trapped in the bone.
Partial Braces (The “2×4” System)
Partial braces are usually used for children who have specific “crossbites” or “underbites.” In this 2×4 system two braces are placed on the back molars and four on the front teeth. This system is used to correct teeth position and to align them properly.

The Financial Reality: Time and Financial Commitments
The most common issue many parents face is the procedure fee. The phase 1 treatment is indeed expensive; however, it also saves parents from higher costs that occur later.
The Cost-Benefit Analysis
- Average Duration: Phase 1 usually lasts for 9 to 12 months; in this time you visit the doctor in 6-8 weeks, meaning there will be few trips to the clinic as compared to traditional braces.
- Avoiding Surgery: Many people wait until the child becomes an adult, resulting in a more expensive process that is maxillofacial surgery, which can cost upwards of $20,000 to $40,000. If parents go for phase 1 for their child, it usually prevents them from future expenses and surgery.
- Shorter Phase 2: Phase 1 is focused on heavy lifting, whereas the phase 2 braces that take place in teenagers are much shorter and less difficult. It also has less cost because the teeth only need minor alignment instead of fully structural movement.
Child Life with Phase 1: Sports, School, and Self-Esteem
Many parents get worried about how a 7 or 8-year-old kid can handle phase 1. At this age the children view braces or expanders as a short-time process; their minds don’t worry much about the process as compared to teenagers’.
Physical Adaptation: The adjustment period lasts for 48 hours, in which a child faces difficulty in swallowing. However, as the days pass, many children even forget the appliance is there.
Sports & Music: Most appliances are compatible; they won’t come out when the child is playing. However, if your child plays a wind instrument, it can be difficult to do for a short period of time, but it won’t stop them from performing.
The “Middle School” Factor: Correcting main mouth issues that are visible before high school is the best thing, as it will save the child from social pressures of middle school that can impact their self-confidence.
What are the benefits of early orthodontic treatment?
Early treatment, like phase 1, is about prevention. The primary benefits include the following:
- Guiding Jaw Growth
- Preventing Impacted Teeth
- Correcting Harmful Habits
- Lowering Trauma Risk
- Improving Speech and Airway
- Simpler Future Care

Common Myths About Early Braces Debunked
Myth: “It’s a waste because baby teeth fall out anyway.”
Reality: It is not a waste because the orthodontist treats the jawbone that holds the teeth. If the bone is too small, there is no space for adult teeth there once the baby teeth fall out.
Myth: “My child will have to wear braces twice, which is unnecessary.”
Reality: 2-phase treatment will only be recommended when the first phase requires extractions of healthy teeth or invasive surgery later.
Myth: “Early treatment is painful for young kids.”
Reality: It is not as painful as parents think because the bone is less dense and the jaw isn’t mature enough. Moving the jaw of an 8-year-old child is easier than doing it on a 17-year-old child.
Frequently ask question by parent on Early orthodontic treatment
Can a child get braces with baby teeth still in their mouth?
Yes, this is known as phase 1, or interceptive orthodontics. The treatment usually takes place when a child is 7 or 10 years old to correct the jaw issues.
How long does a palatal expander stay in?
The active widening takes place for 2 to 3 weeks; however, the appliances stay in the mouth for 6 to 9 months, as it allows the new bone to become permanent.
Does my insurance cover early treatment?
Most dental insurance plans have a lifetime orthodontic maximum. This amount can usually be used for Phase 1, with the remaining balance applied to Phase 2 later.
What is the best age to get braces?
The most common age for having braces is between 11 and 14; however, the best age for orthodontic phase 1 is 7. This allows the orthodontist to examine if a child needs early intervention phase 1 to correct jaw growth or not.
At what age can kids get braces?
Kids can get partial braces as early as 7 or 8 years old if there is a medical urgency like correcting jaws.
When should kids get braces?
Children should get braces when their orthodontist identifies a “skeletal” issue that could become permanent if not treated during a growth spurt. Common issues a child can face are crossbite, an underbite, extreme crowding, or front teeth coming outside.
Conclusion: Setting the Foundation for a Lifetime Smile
Early orthodontic treatment isn’t something to worry about; in fact, it is a clinical advantage of modern dentistry. By visiting an orthodontist when your child turns 7, you are not pressuring them toward braces, but you are helping your child avoid a future painful process. Whether the orthodontist recommends immediate interceptive treatment or a “Growth Guidance” plan, you can stay calm because it comes from professional monitoring. Every child is different, so their face and jaw also develop at different rates. By understanding the main issue earlier, you can prevent future headaches and help your child in getting improved overall health and breathing.
Also Read: Can 1 Year Old Have Honey? Safety Guide & Age Limits
Medical Disclaimer: The content on orangeparenting.com is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider regarding any medical condition or the health of your child. Never disregard professional advice because of something you read here.